As programs make their final preparations for open enrollment (which begins November 15, 2014), the federal government announced several measures that aim to streamline the enrollment process, including design changes to www.healthcare.gov as well as newly developed resources to help consumers navigate re-enrollment into Qualified Health Plans (QHPs) and the redetermination of premium tax credits and cost-sharing reductions. In addition, the Centers for Medicare and Medicaid Services (CMS) proposed a funding methodology for the basic health plan (BHP). Finally, a new report explores coverage opportunities for the LGBT community within the context of same-sex marriage. These and other state and federal implementation updates are discussed in more detail below.
NASTAD is always interested in hearing about specific state processes related to health reform implementation. Please contact Amy Killelea or Xavior Robinson to share activities or specific documents that have been created.
In This Edition
From the NASTAD Blog: The Most Recent Health Reform Posts
back to top >
Federal Implementation Updates
Healthcare.gov Revamped to Streamline the Enrollment Process
- ACTION STEP: Ensure that outreach and enrollment staff are familiar with the new streamlined enrollment application.
On September 22, the Centers for Medicare and Medicaid Services (CMS) unveiled the redesign of Healthcare.gov. The new Healthcare.gov provides a more streamlined user experience for the vast majority of consumers, and can accommodate people whose housing status is transient and/or in transition. The new website features:
- A shorter application for an estimated 70% of new Marketplace applicants;
- Those with specified life circumstances (expected to be 30% of applicants) will complete the standard application
- Fewer mouse clicks to establish an account
- Screening questions and enrollment processes to account for specific life circumstances, including:
- Does everyone applying for coverage have the same permanent home address?
- Is anyone an American Indian or a naturalized citizen?
- Are your spouse and you responsible for a child who lives with you but is not on your federal tax return?
- Do any of your dependents live with a parent who is not on your tax return?
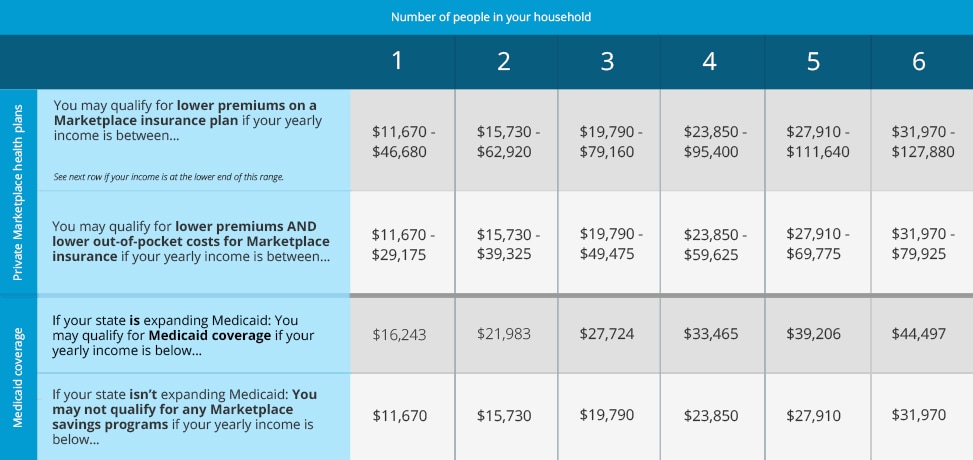
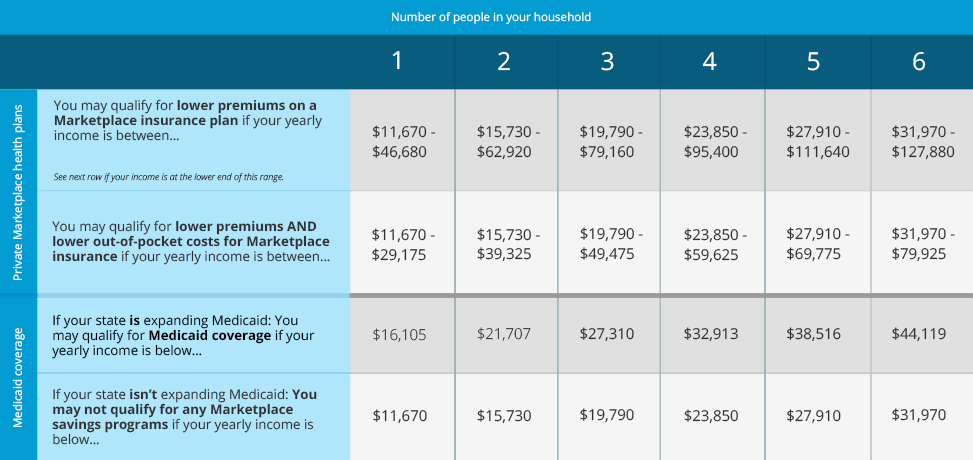
Additionally, Healthcare.gov features new consumer tools and resources that aim to prepare applicants for enrollment into QHPs. These include a one page guide to health insurance Marketplaces; the ability to receive email and text message updates from Healthcare.gov; and a Marketplace application checklist. Healthcare.gov also released the quick reference chart below that differentiates income eligibility for the Marketplace and Medicaid. A complete review of Healthcare.gov can be found in this webinar produced by CMS.
(Click image to enlarge)
back to top >
CMS Releases Resource to Help Consumers Navigate Re-enrollment and Redeterminations
- ACTION STEP: Conduct assessment of Qualified Health Plans (QHPs).
On October 2, CMS convened a webinar to outline the re-enrollment and redetermination process for the 2015 benefit year. The automatic re-enrollment into a QHP, and redetermination of the premium tax credit and cost-sharing reductions occurs when a consumer takes no action to terminate their coverage, or to select a different QHP at the conclusion of the benefit year. CMS highlighted the following key points about the process:
- Between October 1 and November 15, consumers who are currently enrolled in QHPs will receive notices regarding open enrollment and re-enrollment from the Marketplace and their insurance carrier. CMS encourages consumers to review the information that is contained in both notices so they can make informed decisions regarding their health insurance coverage.
- Notices from Marketplaces will focus on key open enrollment dates and deadlines and the re-enrollment and redeterminations process. Marketplace notices will be translated into Spanish for those consumers who indicated that it was the preferred language at the time of enrollment.
- Notices from insurance carriers will inform consumers on whether or not their existing plans will be available in the Marketplace, the 2015 premium expense, and include a reminder of the 2014 premium tax credit and any applicable cost-sharing reductions.
- In federally facilitated Marketplaces and state-based Marketplaces that choose to implement auto-enrollment, consumers who do not terminate their coverage, or select a new plan by December 15 will be automatically re-enrolled into a QHP at their existing level of premium tax credit and cost-sharing reductions. These consumers will receive a notice informing them of their re-enrollment after December 15. All consumers will still have until February 15 to select a new plan. Note: if you are in a state-based Marketplace state, check with your state about whether re-enrollment is automatic.
- Consumers who have not updated their eligibility information by December 15, and have not authorized the Marketplace to contact the Internal Revenue Service will remain at their existing premium tax credit and cost-sharing reduction levels.
- CMS encourages all consumers to review their 2015 Marketplace options. While the re-enrollment and redeterminations processes are important stop-gaps for consumers to maintain coverage, they are no substitute for conducting a thorough plan assessment.
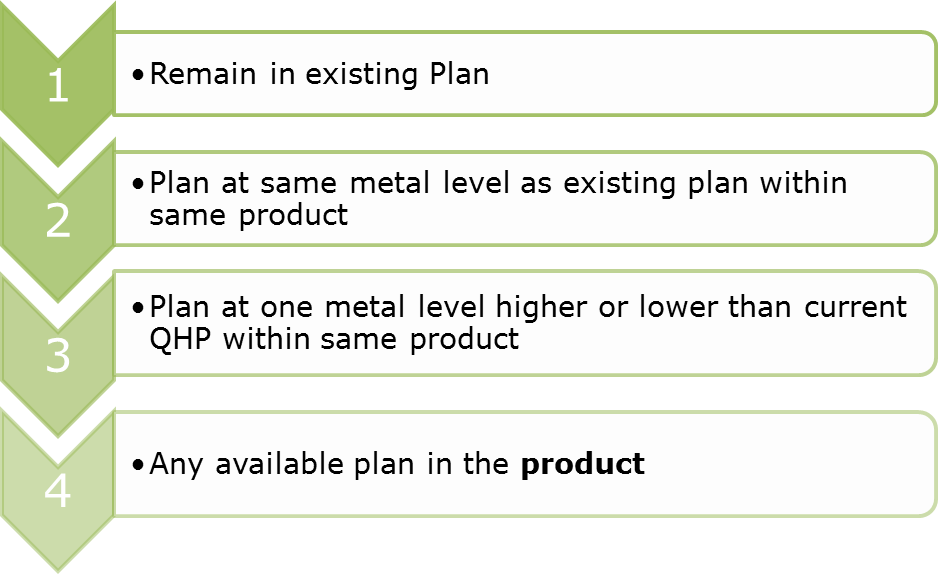
CMS has established a hierarchy of re-enrollment for instances where an enrollee’s QHP or product are no longer available. Of note, a product is a unique set health insurance coverage benefits that an issuer offers using a particular network type within a service area. Examples of types of products include preferred provider organizations (PPOs), and health maintenance organizations (HMOs). An abridged hierarchy is below.
back to top >
Update on Data Matching Inconsistencies
- ACTION STEP: Monitor any outstanding documents clients must submit to keep their coverage.
Consumers who lost Marketplace coverage because they failed to resolve income, and immigration and citizenship data matching issues have 90 days to appeal the decision to terminate their coverage. Individuals with missing income or immigration and citizenship information had until September 30 and October 31 respectively to resolve their data matching issue, or face the termination of their plans and premium tax credit and cost-sharing reductions. While both deadlines have passed, consumers may still submit documents to resolve data matching issues. Those who believe their coverage was erroneously terminated can appeal the decision by contacting their Marketplace.
Inconsistencies can occur when the information reported in a consumer’s application, such as a Social Security or Permanent Resident Card number, is incomplete or different than the information that the government has on file. A data inconsistency does not necessarily mean that there is a problem with an individual’s eligibility for enrollment; but rather that additional information is needed to verify the information provided in an application. Tips on how to resolve a data inconsistency can be found here.
back to top >
HHCAWG Responds to CMS’ Request for Information Regarding Innovative Care Coordination Models
- ACTION STEP: Monitor developments in medical homes and care coordination models in your state.
On November 3, the HIV Health Care Access Work Group (HHCAWG) responded (Attached in Email) to the CMS’ request for information regarding innovative care models. CMS requested that the public offer input and considerations on how it should test innovation in stand-alone Medicare Prescription Drug Plans (PDPs); Medigap and Retiree Supplemental health plans; Medicare Advantage and Medicare Advantage Prescription Drug; and Medicaid managed care plans. Highlights from HHCAWG’s response include:
- Models that pair reimbursement mechanisms with innovative delivery systems that are inclusive of community-based drug user health and harm reduction organizations are of particular importance.
- There are considerations unique to providing services to people living with HIV such as,
- Reimbursement should reflect the cost of care and the complexity of delivering quality HIV services.
- Models that emphasize community providers and public health systems should be a priority.
- Quality measures should include HIV prevention, treatment, and viral suppression metrics.
- States are at the forefront of promoting alignment of provider incentives and quality metrics across managed care plans:
- Washington State has recently launched efforts to coordinate performance and quality measures across public and private payers.
- New York’s Medicaid Special Needs Plan, administered by Amida Care, includes a number of HIV-specific quality measures.
back to top >
State Implementation Updates
Kaiser Family Foundation Releases Issue Brief on Insurance Coverage for the LGBT Community
- ACTION STEP: Monitor state developments on the impact of same-sex marriage on eligibility for services.
On October 23, the Kaiser Family Foundation released an updated issue brief that profiles Health and Access to Care and Coverage for Lesbian, Gay, Bisexual, and Transgender people in the United States. The brief discusses new demographic data within the context of federal policies on health coverage, including the Affordable Care Act, and same sex marriage. Of note, the report estimates that nearly 390,000 uninsured LGBT individuals could qualify for Medicaid in states that plan to expand Medicaid, and that approximately 1.12 million uninsured LGBT individuals could receive subsidies to help with the cost of coverage in Marketplaces.
back to top >
RWJF Study Finds Significant State Variation on Essential Health Benefit (EHB) Benefits
- ACTION STEP: Review your state’s Essential Health Benefits Plan.
- ACTION STEP: Report discriminatory plans to your state’s insurance commissioner.
A new study released by the Robert Wood Johnson Foundation and the University of Pennsylvania found significant state variation in essential health benefits (EHB). The ACA requires the vast majority of private health insurance plans, including QHPs; and Medicaid to cover services within ten broad categories which are depicted in the image below. The study included several key findings:
- While the ACA prohibits dollar limits on all EHB services, most states have implemented other quantitative service utilization limits (e.g., limits on the number of annual doctor’s visits or other services);
- Chiropractic care, home health, skilled nursing, and hospice services are among the most likely services to be limited; and
- The absence of a more rigid national standard contributes to variation.
Please report discriminatory plans to your state’s insurance commissioner. A directory of insurance commissioners can be found here.

Source: Department of Health and Human Services
back to top >
CMS Proposes Funding Methodology for Basic Health Plan
- ACTION STEP: Monitor BHP developments in your state.
- ACTION STEP: Inform NASTAD of developments on the BHP in your state.
On October 22, CMS released a proposed funding methodology for the 2016 basic health plans. The purpose of the BHP is to minimize churn between Medicaid and subsidized Qualified Health Plan (QHP) coverage by allowing states to put in place a public program for people with income between 139 and 200% of FPL. States pursuing this option are examining ways to design a Basic Health Plan that is closely aligned to Medicaid in order to minimize disruptions in care for people whose income may fluctuate between Medicaid eligibility and QHP coverage. States that choose to establish a BHP will receive funding from the federal government which is equal to 85% of the premium tax credits that enrolled individuals would have received had they participated in the Marketplace.
back to top >
NASTAD Updates
NASTAD Convenes Annual National Viral Hepatitis Technical Assistance Meeting
NASTAD convened the annual National Viral Hepatitis Technical Assistance Meeting Washington, DC on October 20 - 22. The meeting provided technical assistance and educational opportunities for health department Viral Hepatitis Prevention Coordinators (VHPC), other health department staff, as well as time for networking with one another and with invited colleagues from the federal government, industry and partner organizations. In addition to health department and community partners, several NASTAD staff shared their expertise and perspective. Presentations from the meeting can be found here.
back to top >
NASTAD Convenes Webinar on Plan Assessment and Enrollment
On August 21, NASTAD hosted a webinar on open enrollment for state HIV/AIDS programs. The webinar was a part of NASTAD’s cooperative agreement with the Health Resources and Services Administration (HRSA), and supported participant efforts to maximize coverage opportunities for ADAP clients during the open enrollment period for QHPs. Discussion included: key enrollment dates and deadlines, re-enrollment considerations, coordination with Medicaid enrollment, and maintaining access to insurance for clients.
back to top >
Health Reform Resources
Information on existing patient rights and protections including prescription medication access is available from CMS. Additionally, the following topic-specific fact sheets are available to help consumers navigate their new insurance coverage:
For questions or to offer suggestions for NASTAD health reform resources that would be helpful to your program, please contact Amy Killelea or Xavior Robinson.
back to top > |